
The Role of Anti-VEGF/Angiopoiten-2 Inhibition for the Treatment of AMD and DME - Episode 2
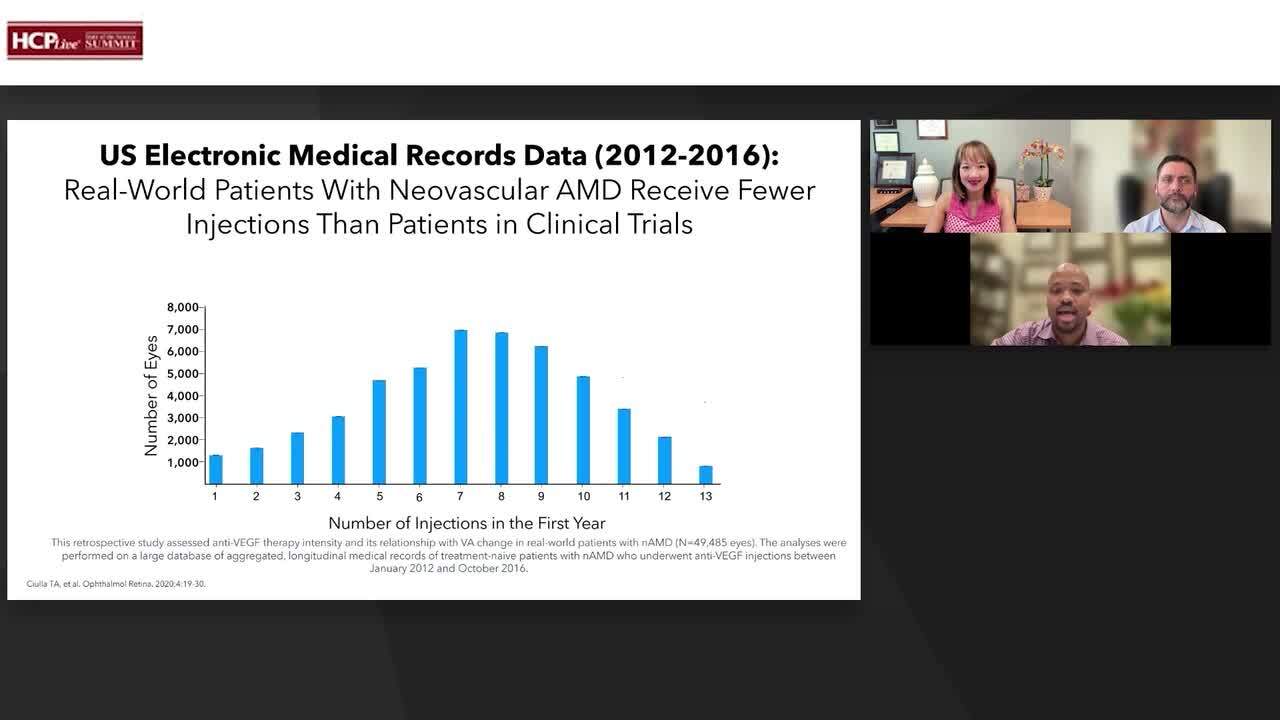
Clinical Trial Overview: Wet AMD
Mark Barakat, MD, discusses the phase 3 TENAYA and LUCERNE trials for patients with neovascular age-related macular degeneration (nAMD).
Transcript
Mark Barakat, MD: This is about TENAYA and LUCERNE, which looked at faricimab dosing up to 16 weeks compared to aflibercept with a regular loading dose and then Q8 week dosing. Essentially, there were OCT and visual acuity criteria for determining if the patients could go Q8 weeks, Q12 weeks, or Q16 weeks on the faricimab dosing. So akin to, if you want to say, a more rigorous treat-and-extend that we do in the clinic. You want to make sure that the anatomy matches the vision, and the vision matches the anatomy. And you'll see this, again, this nice response in both the faricimab arm and blue and the aflibercept arm, and we're very lucky that aflibercept is a great drug. We can see it here, as well. And you see that they have a nice response all the way through week 48, but with fewer doses of the faricimab. This is just a percentage of patients with absence. So basically, are they dry? It's not just a question of the CFD, which is a number that I may not even look at in the clinic. I may look at just the anatomy. And if you look, weeks 4, 8, 12, and 48, it's actually in favor of the faricimab arm in terms of it being dry in terms of absence, somewhere between 60% and 77%, and with the aflibercept arm you get somewhere between 47% and 67%.
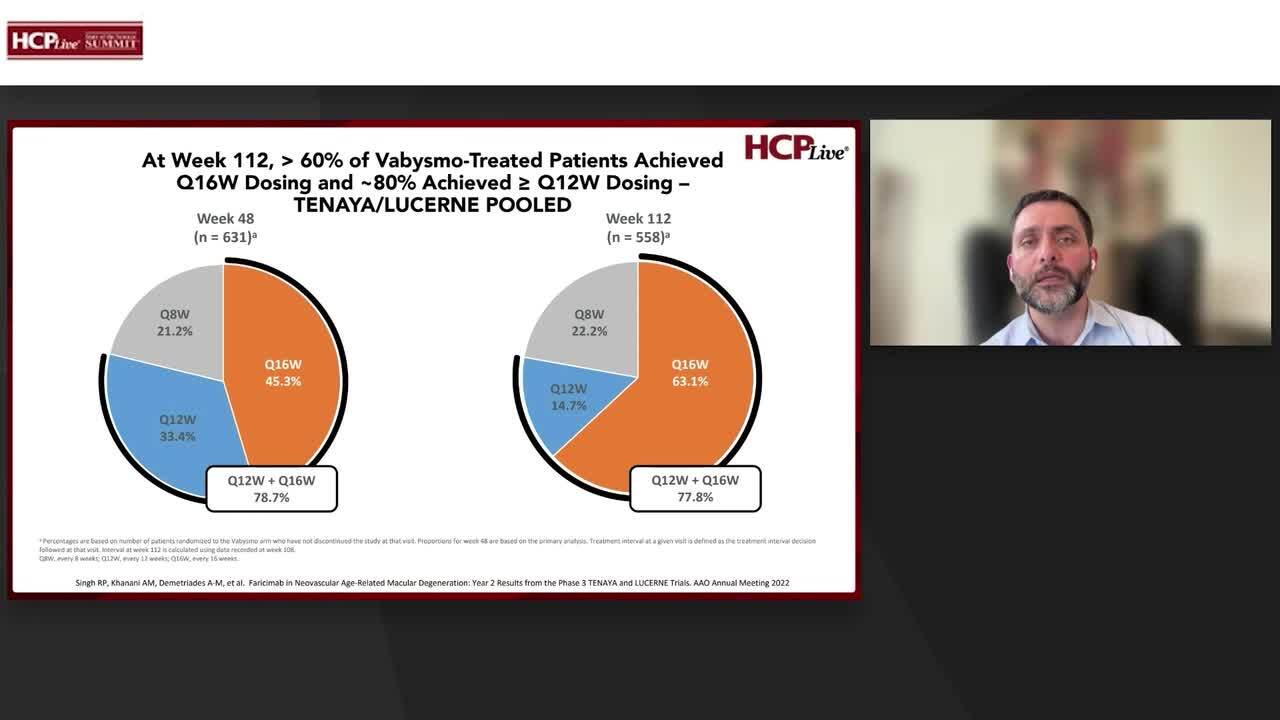
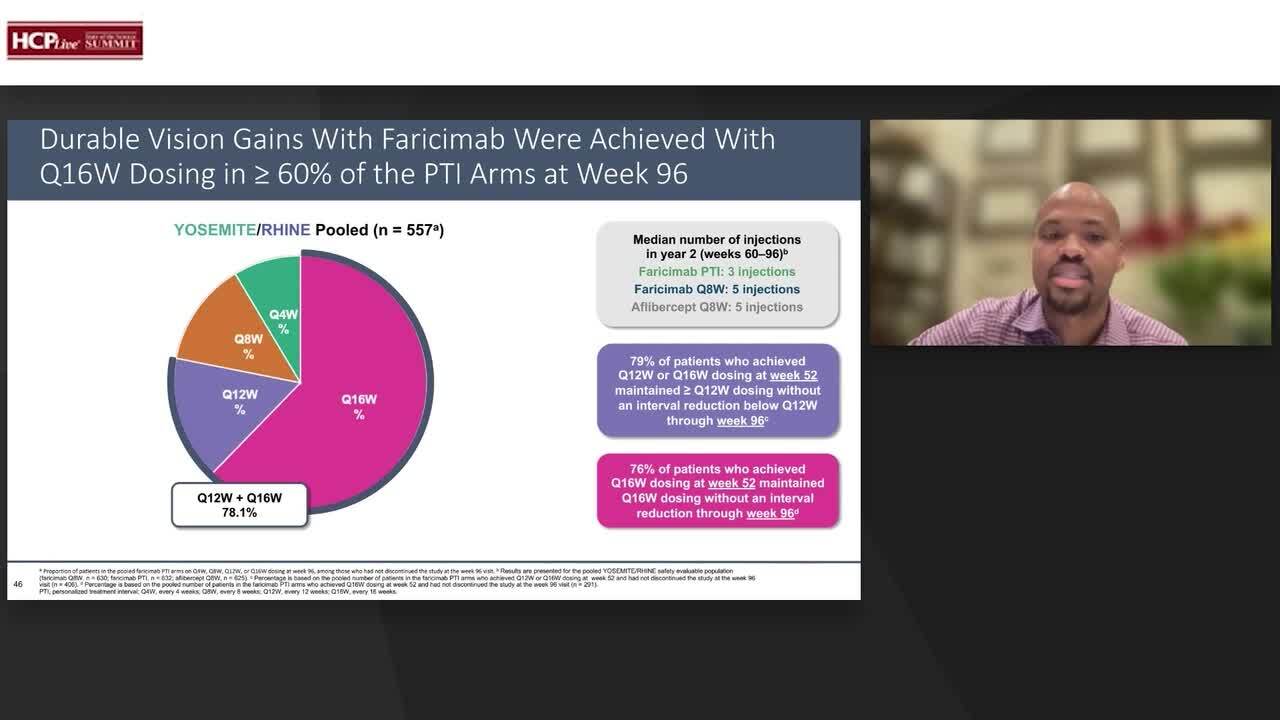
These are the key results. We talked about on the left-hand side, we talked about the vision. In the middle, we talked about anatomy. On the right-hand side, we talked about something that we care very deeply about as clinicians. How many of these patients can stay about 12 to 16 weeks? About 80 percent. This is the anatomy. As you can see here, nice stability throughout in both TENAYA and LUCERNE, all the way through week 112. Now, interestingly, if you look at year two, right, this is not, again, being achieved with 6 injections of aflibercept and 3 injections of VABYSMO. So there's a difference. Comparable proportions of patients gained or avoided loss. So, you know, the same thing we talked about before, different ways of looking at it. The majority of patients in TENAYA are roughly 90% in both the aflibercept arm and the faricimab arm maintain vision, meaning didn't lose three lines. Same thing with LUCERNE, and it's about 20% or so in both trials, in both arms, over three line gainers. So, again, a nice response. Here it is. Greater than 60% of faricimab patients achieved Q16 weak dosing at the snapshot, at week 112. So, basically, if you continue with these patients to be flexible in terms of the treatment regimen, as you can see, 74%, 81% can go to Q12 to Q16. So, this here is going to be the vision gains baseline with Vabysmo. Up to 16 weeks, they were comparable, and this is pooled. Just to keep it equal, because I showed you the year one in pooled. This is very encouraging.
Now, if you want to get a little bit more granular, you ask yourself the heat map on the left-hand side. So, if you look at the greenest initiation period, and then if you look at the purple is Q12, and the pink is Q16, and you see the line, the dividing line in the middle of year one. So, we know the ones that are highlighted in the green box right there are the patients that at year one, they got to 16 weeks. weeks. End of story, right? Because it's a one-year disease, we know that. The question is, how many of them actually stayed at 16 weeks? the majority, about 70%. And if you look at the anatomy, if you look at the vision to the right, you'll see that they stayed, they were nice and stable. Well, great. Well, how about those patients that weren't lucky enough or well-treated enough at year one? They were not at 16 weeks, but they were 12 weeks, because life's a bell curve. How did they do? Well, if you started at 12 weeks at year 1, at year 2, again, the majority were either at 12 or at 16. Some of them stretched out, we look at 60%. Again, nice anatomy. And you can extrapolate that to those folks that need a more frequent injections. Of course, I wish I could say that for SNAP, everyone is on Q12, we know better than that. There are some that need Q8, but thankfully, for people that needed Q8 treatment at year one, the majority of them were actually on increased dosing interval by the end of year two. So, you know, to Diana's point, we have to treat, we have to treat rigorously, but that doesn't necessarily mean that we always have to maintain the same interval because we have data here that shows that you can extend and safely, as you can see on the right-hand side.
Speaking of safety, safety is foremost in all of our minds. We do no harm. This was very well tolerated. If you look at the safety results in both the faricimab arm on the left, the aflibercept arm on the right, it was well balanced. And we always worry about inflammation. There really was no inflammatory signal of note. Of course, there were cases of endophthalmitis.
In summary, we have good data now about individualized dosing up to 16 weeks in control of anatomy, in control of vision, in patients who years, two years of follow-up in macular generation and the important thing is this is not new we know we can do this we know we can do this is a monthly injection so we know we can do this is a bi-monthly injection but this was done with about 80% of solo patients at Q12 week injection and 60% at Q16 injection, so well tolerated, and as we'll hear later from Matt we'll talk about the long-term extension study and other studies as well so there is a commitment to actually further follow-up to help us understand these new molecules better.
Transcript is AI-generated and edited for clarity and readability.


