
The Role of Anti-VEGF/Angiopoiten-2 Inhibition for the Treatment of AMD and DME - Episode 3
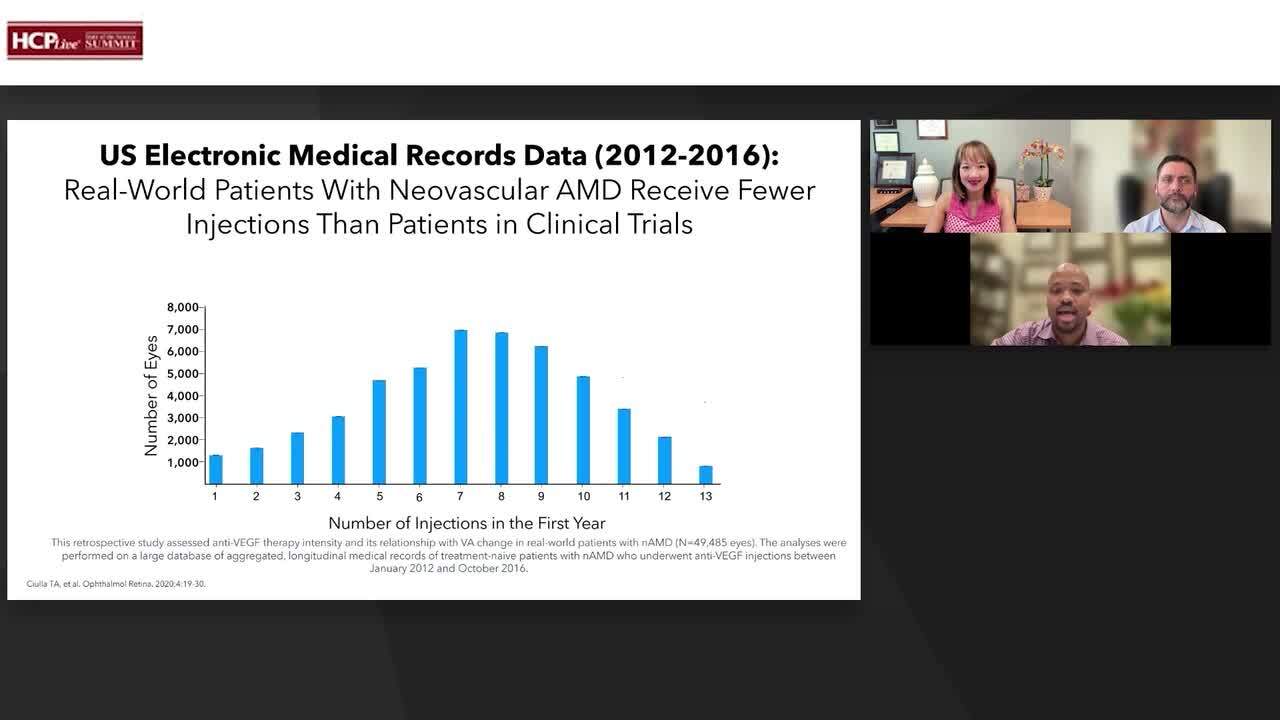
Clinical Trial Overview: DME
Matthew Cunningham, MD, FASRS, provides the highlights of the YOSEMITE and RHINE trials for patients with diabetic macular edema (DME).
Transcript
Matthew Cunningham, MD: YOSEMITE and RHINE actually had 3 arms, so these were both identical phase three randomized double-masked trials compared to aflibercept. The study involved patients with diabetic macular edema (DME) greater than 325-micron CST, and vision had to be 20/40 or worse.
There were 3 arms that patients could get randomized into. Two of them were faricimab arms, and one was the comparator of aflibercept every 8 weeks. Within the faricimab arms, the patients either received 6 loading doses followed by Q8-week intervals, and that was through the end of the study at 2 years, or they were in the PTI (Personalized Treatment Interval), which Mark basically alluded to as almost like their protocol-driven treat-and-extend interval. This treat-and-extend dosing regimen, which we could go into in a little more detail, had intervals that adjusted from either Q4 weeks all the way up to Q16 weeks. This was based on CST values and BCVA changes at the active dosing visit. This was changed throughout the entire study based on what their visit looked like the time before.
We found that number one, faricimab met its endpoint, which was non-inferiority at year 1. You can also see that this is the data through the end of the study. The data showed that visual gains were equivalent among all 3 groups, both the PTI arm, the Q8-week faricimab, and the Q8-week aflibercept arm. When we look at the CST reduction, you can see that there is a greater trend toward greater drying in the DME patients on both the faricimab Q8 and the PTI arms through year 1 and 2.
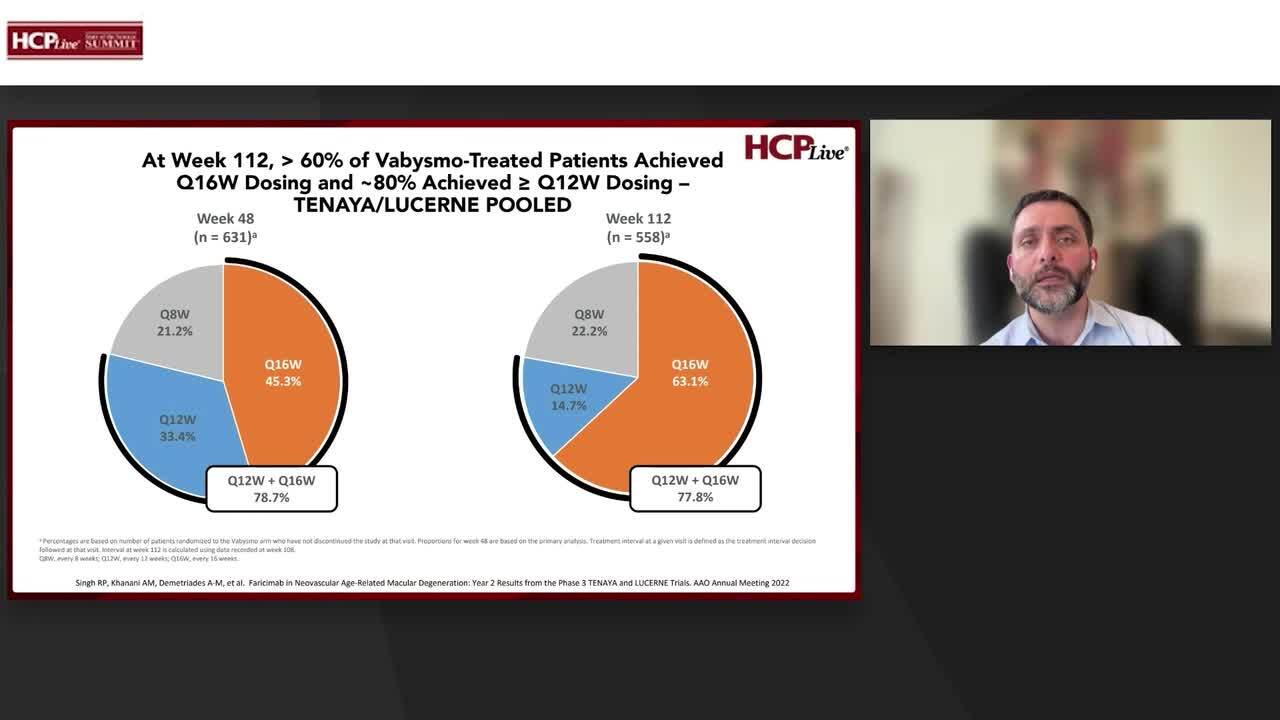
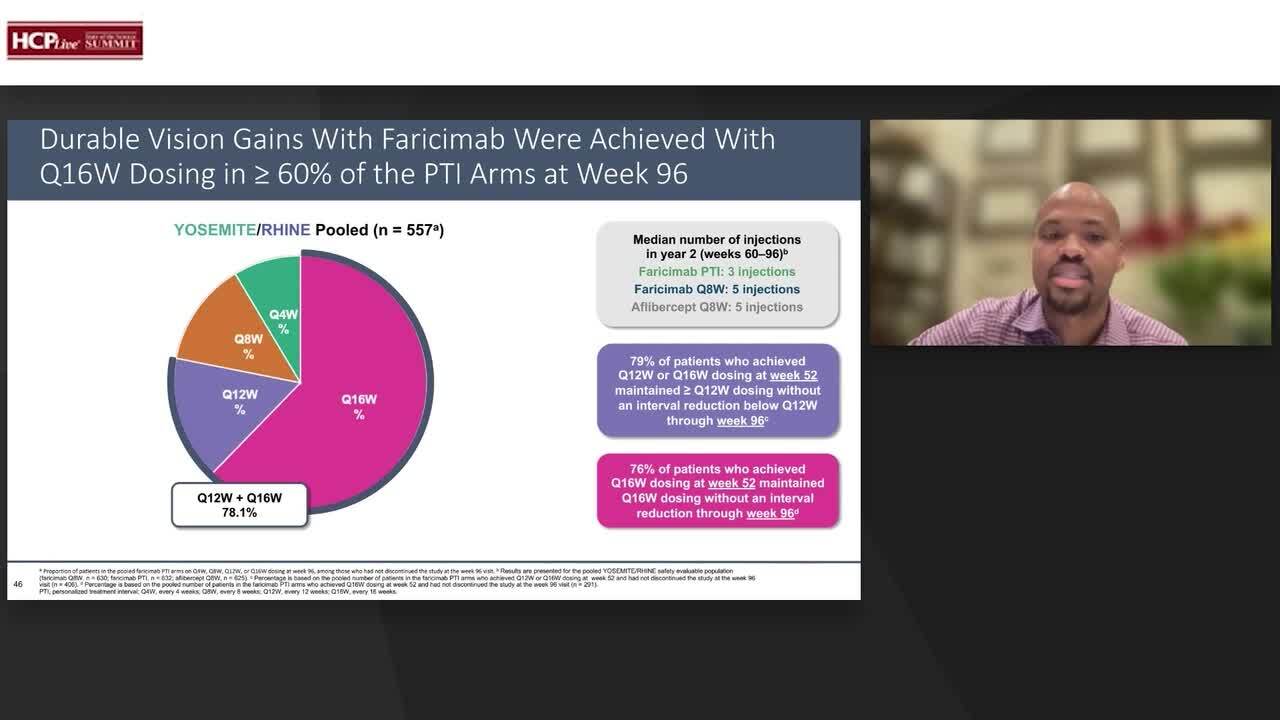
I think the most impressive data comes with the patients that are able to get out to Q16-week intervals and Q12-week intervals. We see that during the pooled data, greater than 60% of patients are in the Q16-week at the end of the study. And when we talk about the median number of injections, Mark alluded to the reduction of injections, especially in year 2 in the TENAYA and LUCERNE, we see the exact same thing in this YOSEMITE and RHINE study, where we see in year 2, the faricimab arm and the PTI only received 3 injections as a median versus 5 injections in the comparator aflibercept arm.
We also see that 79% of patients who achieved Q12-week or Q16-week at the one-year mark maintained over 12-week interval dosing, and that stayed through to the end of the study. And lastly, we see that 76% of patients who achieved Q16 weeks at the 1-year mark maintained this Q16 week without an interval reduction through the 2-year mark.
So let's talk about patients with the absence of DME. Absence of DME was just recorded as less than 350 microns. And you can see here that both arms of the faricimab or Vabysmo compared to the aflibercept had a greater percentage of patients with the absence of DME throughout year 1, and this extended through year 2.
But when we talk about looking at the OCT and just seeing a bone-dry OCT, so zero evidence of any intraretinal fluid, we see that those percentages are lower throughout all arms. However, the trend is for a greater drying effect in both arms of the faricimab compared to aflibercept. I do think that both of these arms or both of these studies showed just the importance of that durability that we've been talking about with faricimab compared to aflibercept without causing any reduction in visual gains. And I think this is a part of what we were discussing in terms of our patients who are trying to get that treatment burden down. If we are able to help our patients out by actually decreasing their treatment burden and extending these visits without necessarily compromising their vision gains, that is the Holy Grail.
Transcript is AI-generated and edited for clarity and readability.


