
Treatment Resistant Depression - Episode 1
The Impact of Depression and Treatment Overview
Brent Necaise, MD, reviews incidence and risk factors of depression, as well as the challenges associated with treatment.

Transcript
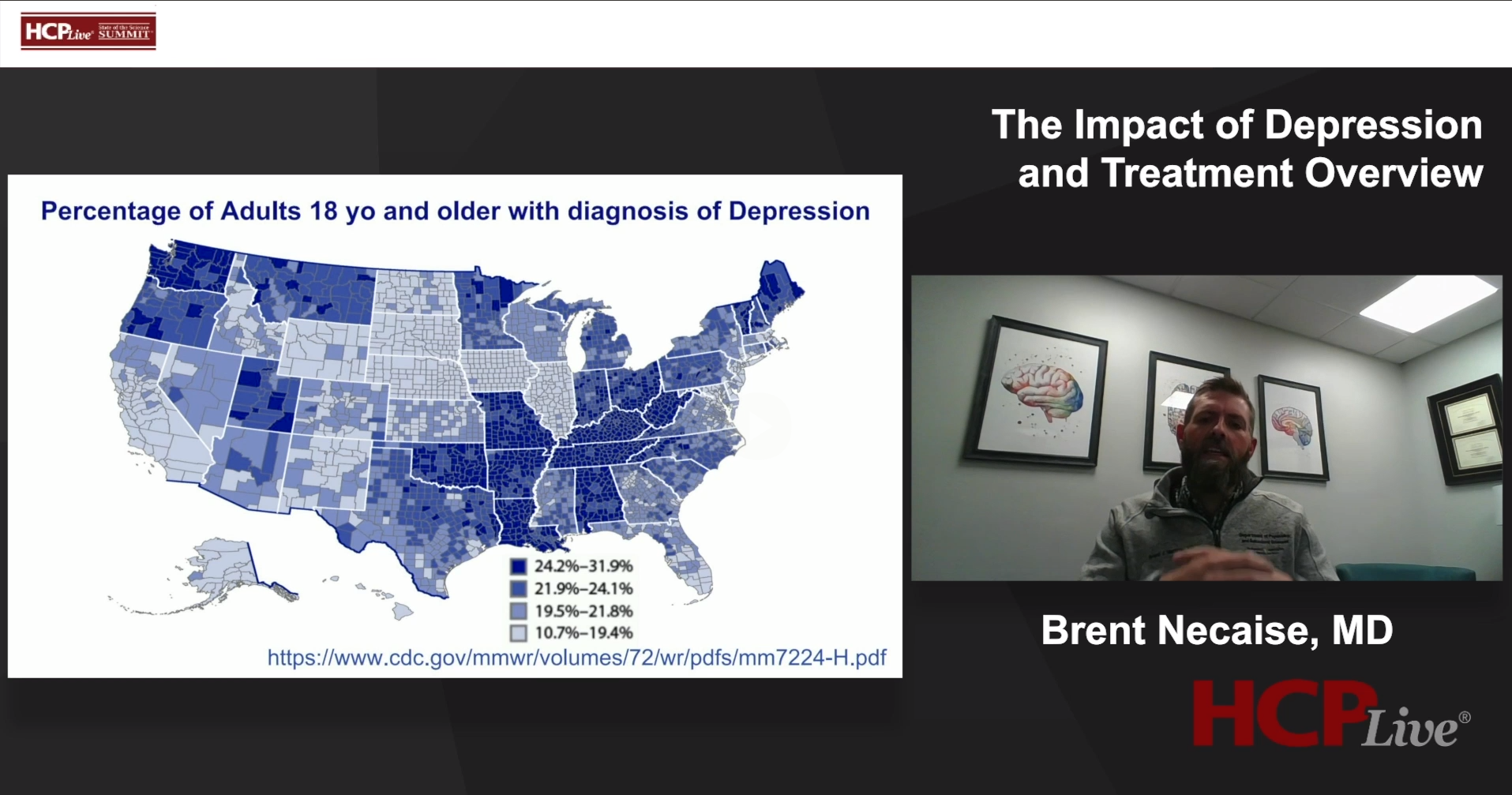
Brent Necaise, MD: Depression is quite a burden on individuals, [on] patients worldwide, but particularly in our country. Here you can see a recent map that was put out by the CDC showing the percentage of adults, 18 years or older, that have been diagnosed with depression, broken down by individual counties and states. As you can see, the South has very, very high percentages of adults who have been diagnosed with depression. Particularly here in Nashville, you can look at the map. Tennessee is in that darkest blue, where 24.2 to 31.9% of adults 18 or older have been diagnosed with depression.
Depression is the leading cause of disability in the United States. Worldwide, it's also a major contributor to the overall global burden of disease. Globally, more than 280 million people of all ages suffer from depression. So, it's quite common and probably more common than what we realize, given that many patients go under diagnosed or undiagnosed. In terms of incidents and risk factors, you can see quite high [incidences] in the South, particularly here in the state of Tennessee. Females carry a higher risk than males, of about 50 percent. Another risk factor would include race. Levels of depression are highest among individuals of mixed race or biracial race, Native Americans, Indian or Native Alaskans and Caucasians. Being African American is protective against depression. Risk factors also include age. Patients who are between 18 and 25 are at the highest risk. Poverty and low education opportunities also convey increased risk. Individuals who identify as a sexual or gender minority, members of the LGBTQI+ population, experience depression at much higher rates. And then again, southern states have much higher rates of depression, which correlates with higher rates of obesity, heart disease, stroke, sleep disorders, as well as just overall lower access to medical care. Is there a causal link? We're not sure, but it's pretty clear that there's definitely a correlation.
So let's talk about treatment as usual, what [are] the common protocols that we have for treating patients who present with us with depression. We'll start with the good news. This comes out of the Star*D trial, which is a really pivotal study in the area of depression treatment.
The good news is that [if] a patient comes to us meeting the criteria for major depression, let's say it is their first episode of depression, and we start an antidepressant for them, we know that 30% will have complete resolution of their depressive symptoms [and] they will go into remission. So roughly a third [of patients]. An additional third will have an improvement in their symptoms, they'll respond. What we mean by respond is that, of the objective assessments of the severity of depression, their scores would decrease by 50%. Not to the point where they would be considered free of depression, but [they experience] a significant improvement in their symptoms. So that's the good news. [If] a patient comes to us depressed [and] we start a medication, there's two thirds percent likelihood that their symptoms will improve. Of that group, overall, half of them will have a remission.
What happens to the other third? Well, that's the bad. With the first treatment of a standard medication for depression, the last third will fail to show any clinical response. We would not see any significant improvement in their depressive symptoms. Additional bad news is that with each additional treatment trial (eg, the first medication failed, we try a second medication), remission potential continues to fall and the risks of side effects continue to increase. At this point About 40 % of patients, if not more, will discontinue their medications on their own within three months There's very high rates of patients not sticking to the medications and continuing to experience depressive symptoms.
Now for the ugly. Under treatment is very common with patients presenting for depression. What [do] I mean by under treatment? These are patients who are either under diagnosed or inadequately treated. In many studies, 20 to 30% of patients who are receiving treatment are receiving inadequate treatment. The most common example would be a patient is started on a subtherapeutic medication antidepressant that's never increased to a therapeutic dose This often happens by non-psychiatrists who are not as familiar and as experienced with these medications. Usually, the ways around this would be a collaborative relationship between primary care and a psychiatrist or psychiatric team. This is also pretty prevalent in rural and underdeveloped areas where there's difficulty to even access care, where there's just not enough care to meet the demands of the people living in those areas. In those cases, many patients Are minimally treated or they've received no treatment at all.
Transcript was AI-generated and edited for clarity.


